Case Study: Neo or No Neo?

A 56-year-old Haitian female presented with complaints of bilateral blurred vision. Her medical history was significant for sickle cell trait, hypertension, hypercholesterolemia, and diabetes mellitus of unknown duration. Her most recent blood glucose level was 180 mg/dL, with a hemoglobin A1c of 11%. Entrance testing was unremarkable. Best-corrected visual acuity measured 20/20 in the right eye (OD) and 20/400 in the left eye (OS). Slit-lamp biomicroscopy revealed mild cortical lens changes bilaterally. There was no evidence of iris neovascularization, and gonioscopy was negative for neovascularization of the angle. Intraocular pressure measured 20 mmHg OD and 22 mmHg OS by Goldmann applanation tonometry.
Fundus examination revealed pink, well-defined optic nerves bilaterally without evidence of neovascularization of the disc. There was extensive lipid exudation with associated macular edema in both eyes, along with numerous dot-and-blot and flame-shaped hemorrhages involving the posterior pole and extending into the equator bilaterally. The retinal arterioles appeared attenuated with arteriovenous crossing changes and an increased arteriolar light reflex, and findings were consistent with hypertensive and arteriosclerotic changes.
Additionally, diffuse exudation was noted throughout the equator, with a coinciding orangish-pink retinal hemorrhage observed superiorly in the right eye. Areas of anomalous retinal vasculature were identified in the inferotemporal and superonasal quadrants of the right eye. Overall, the clinical presentation was suggestive of a multifactorial retinopathy, most consistent with diabetic retinopathy with contributory sickle cell retinopathy.
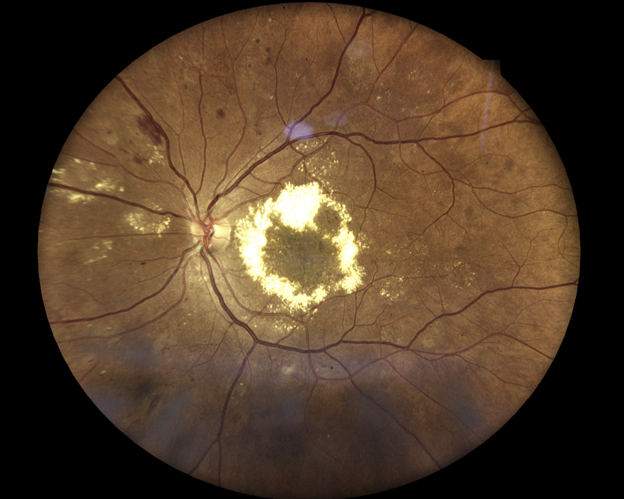
Figure 1 (OS): Significant circinate exudation and macular edema (OS). Scattered dot-and-blot hemorrhages, flame-shaped hemorrhages, and exudates throughout posterior pole and equator.
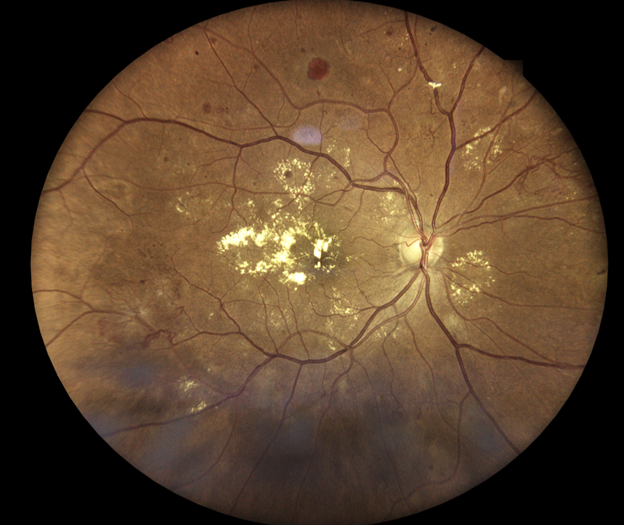
Figure 1 (OD): Macular exudates with macular edema (OD). Exudates, dot-and-blot hemorrhages throughout posterior pole and equator. Anomalous vasculature SN and IT. Orange/pink hemorrhage superiorly.
Optical coherence tomography (OCT) and OCT angiography (OCT-A) were performed using the Optovue Solix by Visionix to assess for the presence of neovascularization and macular edema. Due to the equatorial location of the anomalous vasculature, 9x9 and 12x12mm OCT-A were selected.
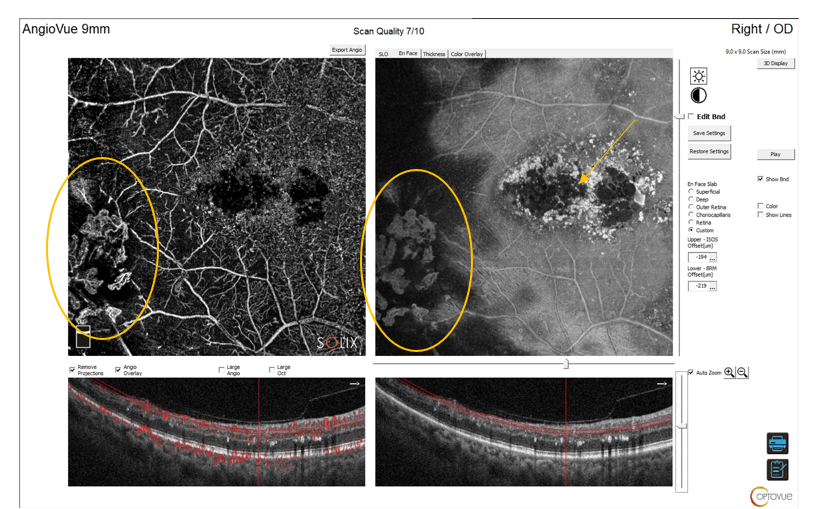
Figure 2: 9x9 mm OCT/OCT-A: Retinal neovascularization visible on OCT-A angiogram and en-face image. Macular edema (exudate) seen on en-face cut (arrow).
 Figure 3: 9x9 mm OCT/OCT-A: Custom slab at the vitreoretinal interface beautifully highlights the neovascular fronds.
Figure 3: 9x9 mm OCT/OCT-A: Custom slab at the vitreoretinal interface beautifully highlights the neovascular fronds.
 Figure 4: 9x9mm OCT-A reveals significant macular edema (exudation and hemorrhages) on OCT b-scan. Diffuse capillary non-perfusion and neovascularization (at border of perfused and non-perfused) retina is visible on OCT-A.
Figure 4: 9x9mm OCT-A reveals significant macular edema (exudation and hemorrhages) on OCT b-scan. Diffuse capillary non-perfusion and neovascularization (at border of perfused and non-perfused) retina is visible on OCT-A.
 Figure 5: 12x12 mm OCT/OCT-A (OD) Illustrates extent of capillary non-perfusion extending into equatorial region.
Figure 5: 12x12 mm OCT/OCT-A (OD) Illustrates extent of capillary non-perfusion extending into equatorial region.
The utilization of OCT angiography was instrumental in confirming the diagnosis of proliferative diabetic and sickle cell retinopathy and identifying associated macular edema. Employing advanced imaging technologies enhances diagnostic accuracy and supports improved clinical decision making.
OPTOVUE SOLIX BY VISIONIX
- The ONLY OCT with FDA-cleared OCT-A metrics
 FullRange® Retinal 16x6.25mm scan
FullRange® Retinal 16x6.25mm scan- FullRange® Anterior Chamber 18x6.25mm scan
- Ultra-fast 120kHz scan speed
- Higher scan density & precision vs. other OCTs/OCT-As
- Integrated fundus camera
- External color & IR imaging
- New optional Topography Module available!
This article originally appeared in Optometric Management's OCT Insights in March 2026: https://optometricmanagement.com/issues/2026/march-april/neo-or-not-neo-widefield-oct-a-reveals-hidden-neovascularization/
 Dr. Julie Rodman is the Chief of the Broward Eye Care Institute in Fort Lauderdale, FL and a Professor of Optometry at Nova Southeastern University. Her research interests include OCT/OCT-A and Vitreoretinal Disease. Dr. Rodman has authored over thirty publications with an emphasis on retinal disease. She recently published “Optical Coherence Tomography Atlas: A Case Study Approach,” the first reference book on this topic written by an optometrist. Dr. Rodman is a member of the AOA, AAO, FOA, and ORS. She has been the recipient of numerous teaching awards and was recognized as a Primary Care Optometry News “Top 300” Optometrists and “Newsweek Best Optometrists of 2021.”
Dr. Julie Rodman is the Chief of the Broward Eye Care Institute in Fort Lauderdale, FL and a Professor of Optometry at Nova Southeastern University. Her research interests include OCT/OCT-A and Vitreoretinal Disease. Dr. Rodman has authored over thirty publications with an emphasis on retinal disease. She recently published “Optical Coherence Tomography Atlas: A Case Study Approach,” the first reference book on this topic written by an optometrist. Dr. Rodman is a member of the AOA, AAO, FOA, and ORS. She has been the recipient of numerous teaching awards and was recognized as a Primary Care Optometry News “Top 300” Optometrists and “Newsweek Best Optometrists of 2021.”
**The information provided is for general informational purposes only. It is not intended to replace and should not be considered a substitute for professional medical advice, diagnosis, or treatment. The content is not designed to replace the relationship between a patient and their healthcare provider. Any medical decision should be made in consultation with a qualified healthcare professional who can provide information tailored to your individual situation. Medical procedures, case studies, and practices mentioned in this content may vary depending on regional standards, local regulations, and the discretion of the healthcare provider. The views and experiences expressed are those of the individual user. They may involve off-label use of the medical device, which is not endorsed or approved by the manufacturer. What may be considered appropriate and ethical in one country may differ in another. The content may include general references to medical practices, medications, or treatments that are widely accepted in certain regions but may not be universally applicable or approved. It is important to consult a healthcare professional in your jurisdiction to ensure that the information is relevant to your specific situation. The authors, editors, and contributors of this content disclaim any liability for any adverse effects resulting directly or indirectly from the information contained herein. Readers should exercise their own judgment and seek advice from healthcare professionals when necessary. By accessing and using this content, you acknowledge and accept the terms of this disclaimer.